Left Heart Evaluation
Anatomy & Normal Values
-
LV diameter (diastole): < 5.2 cm
-
LV wall thickness (diastole): < 1.2 cm
-
Left atrial diameter: < 4.0 cm

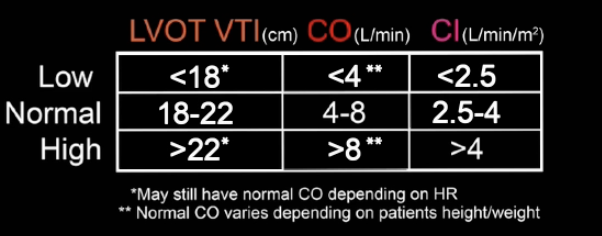
Cardiac Output
-
CO = Stroke Volume × Heart Rate
-
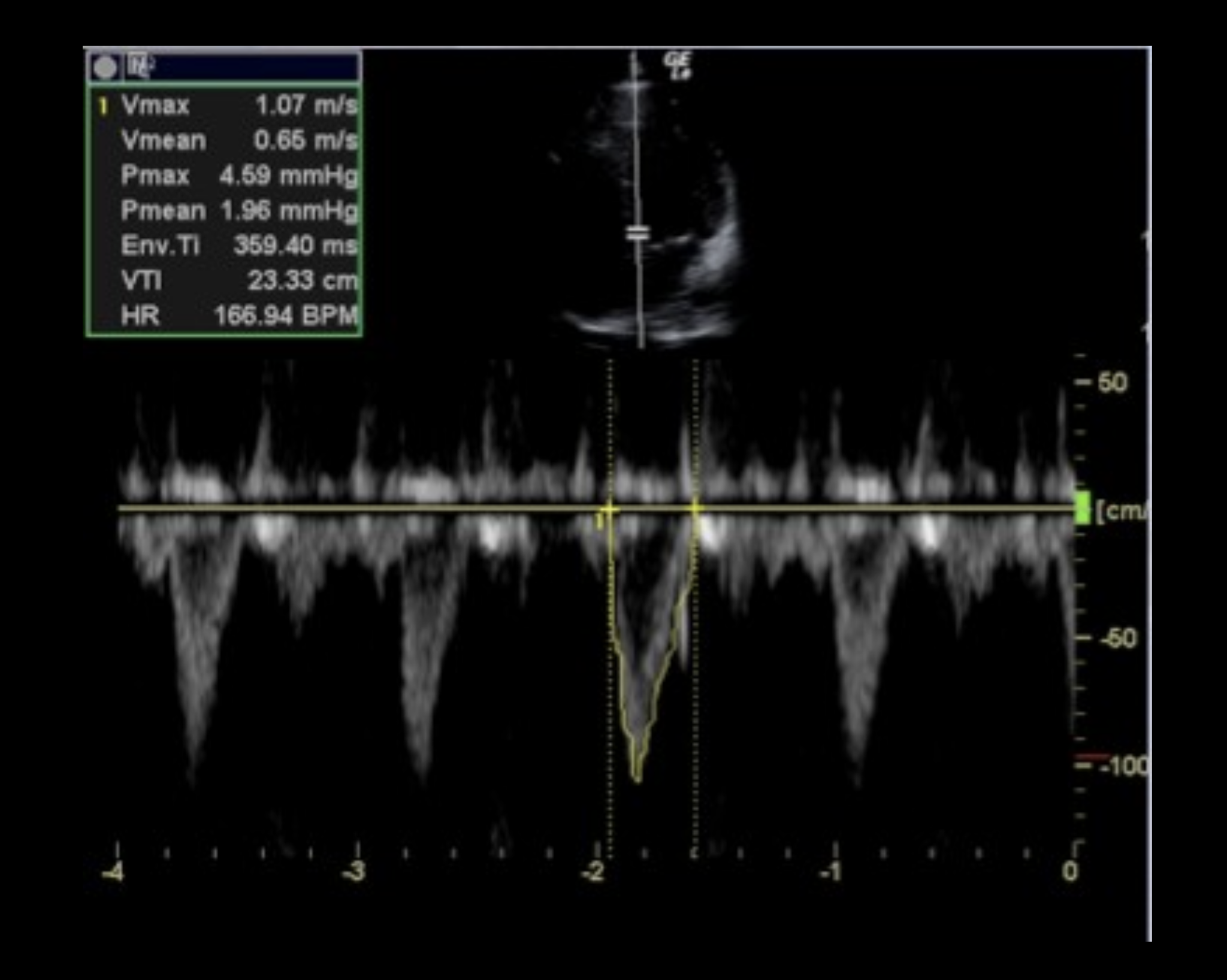
Stroke Volume = LVOT Area × VTI
-
LVOT Area = π × (LVOT diameter/2)²
-
VTI measured via PW Doppler in Apical 5-Chamber or Long Axis view
-
Tips for VTI Measurement
-
Optimize gain, baseline, and sweep speed
-
Measure over several cardiac cycles (especially in atrial fibrillation)
-
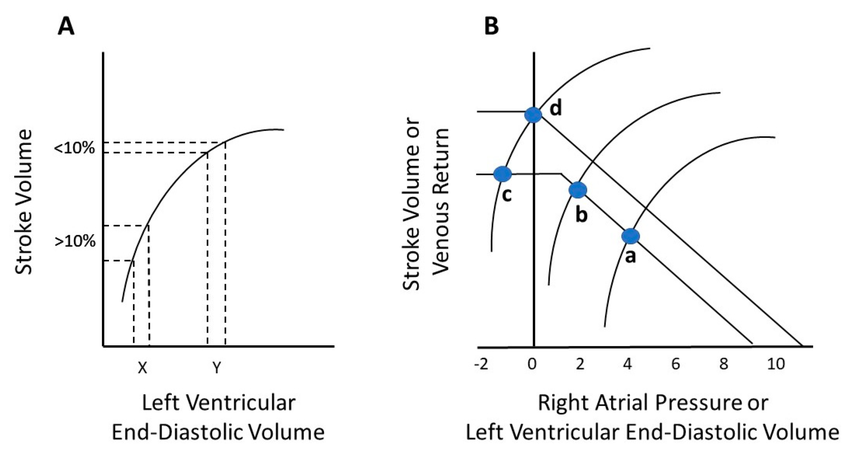
Use passive leg raise (PLR) or fluid bolus to assess volume responsiveness
-
>10% increase in SV or >15% increase in VTI → fluid responsive
-
Ejection Fraction (EF) Assessment
-
Visual estimation: Normal 50–70%, Hyperdynamic >70%, Severe <30%
-
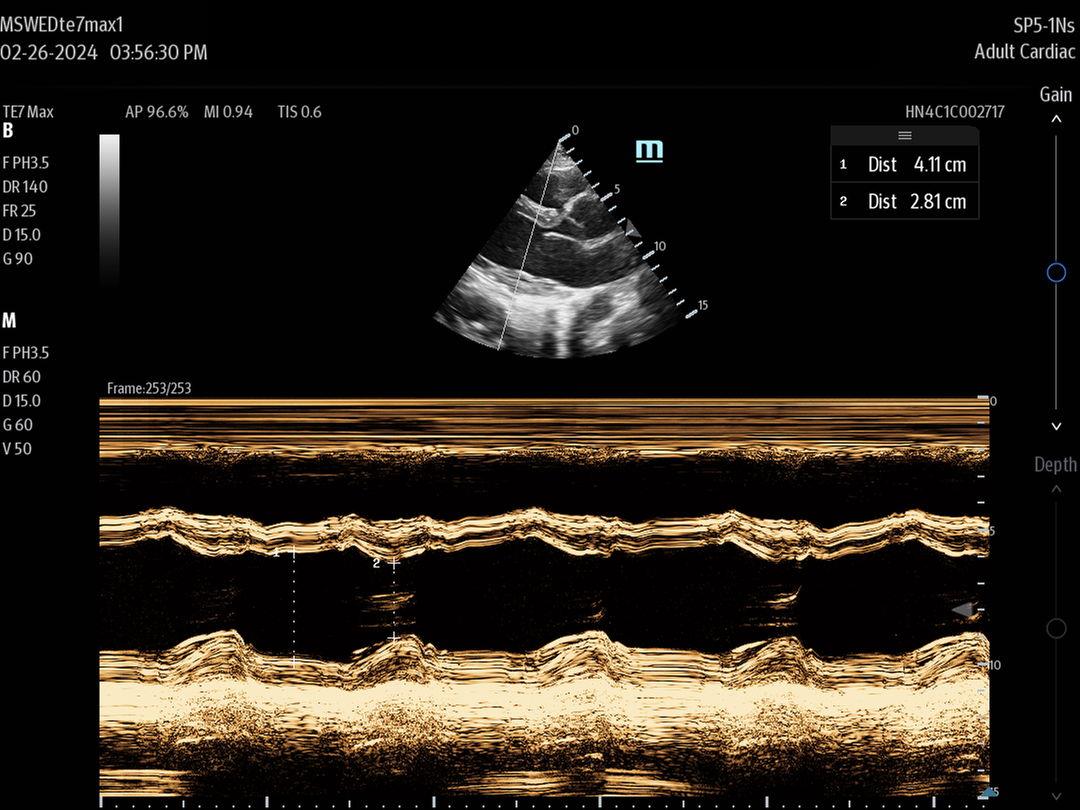
EPSS (E-point septal separation):
-
<7 mm = normal EF, >10 mm = low EF
-
EF ≈ 75.5 − (2.5 × EPSS)
-
-
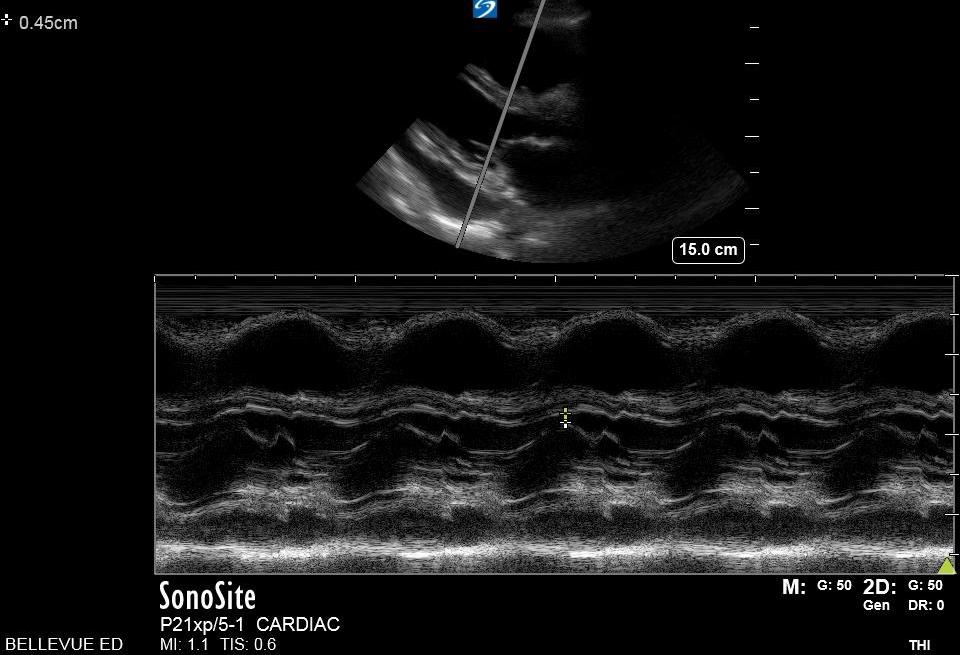
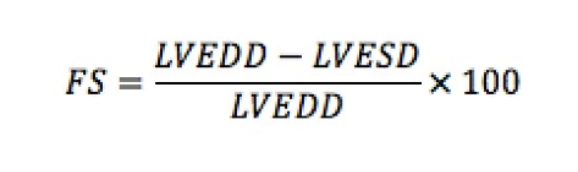
Fractional Shortening (FS):
-
Normal: 25–45%
-
FS ≈ ½ of EF; less reliable with regional wall motion abnormalities
-
-
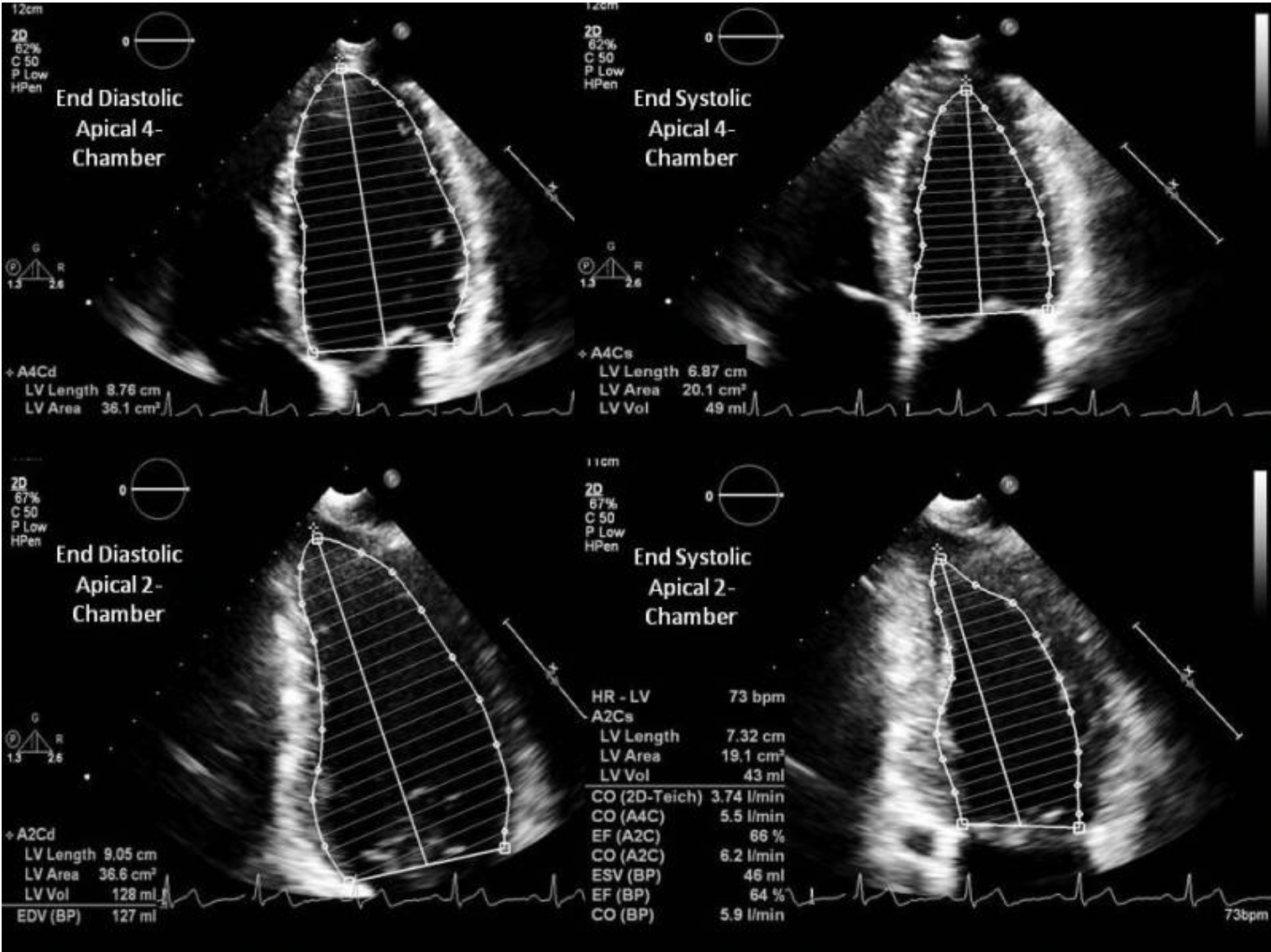
Simpson’s Method (Method of Discs):
-
Most accurate; requires A4C & A2C views + software
-
EF = (EDV – ESV) / EDV × 100



Right Heart Evaluation
Anatomy & Measurement
-
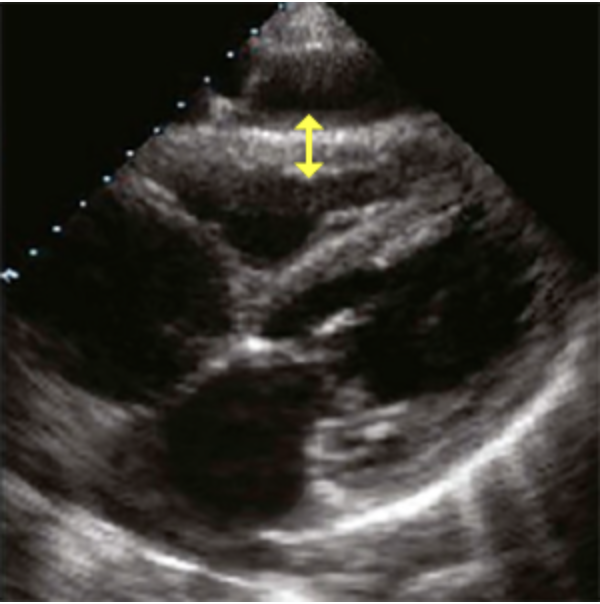
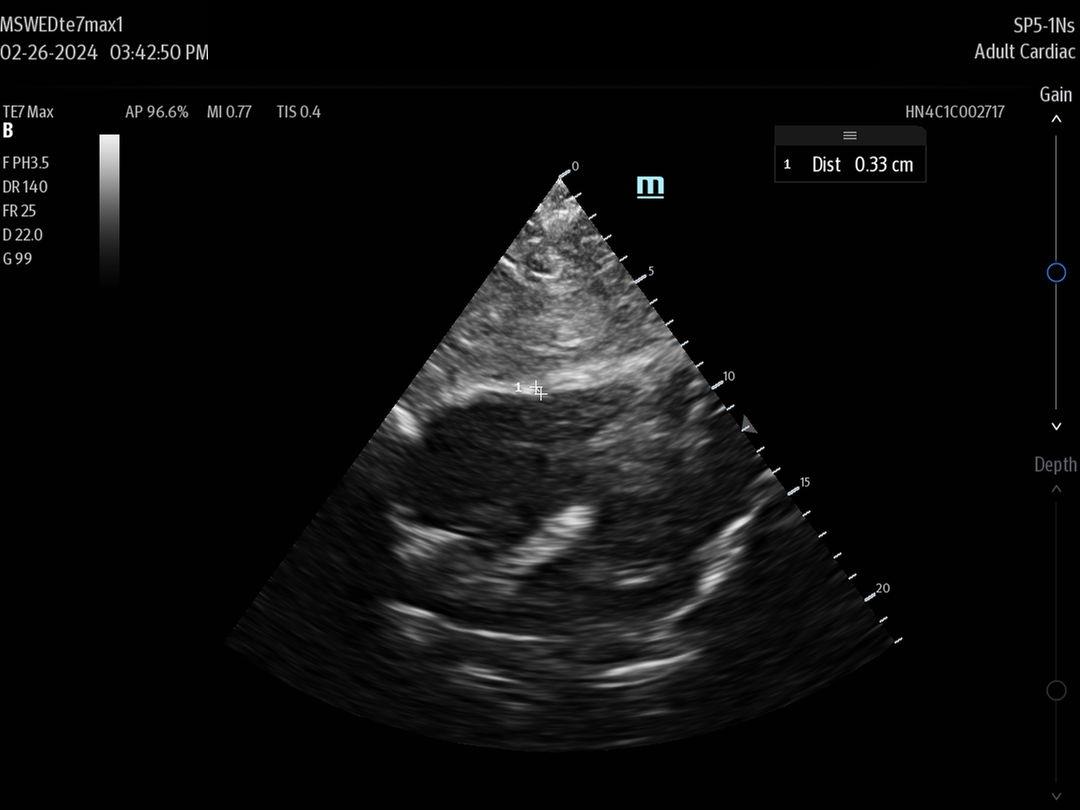
RV Free Wall Thickness: <5 mm (measured in diastole, subxiphoid view)
-
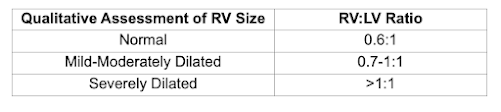
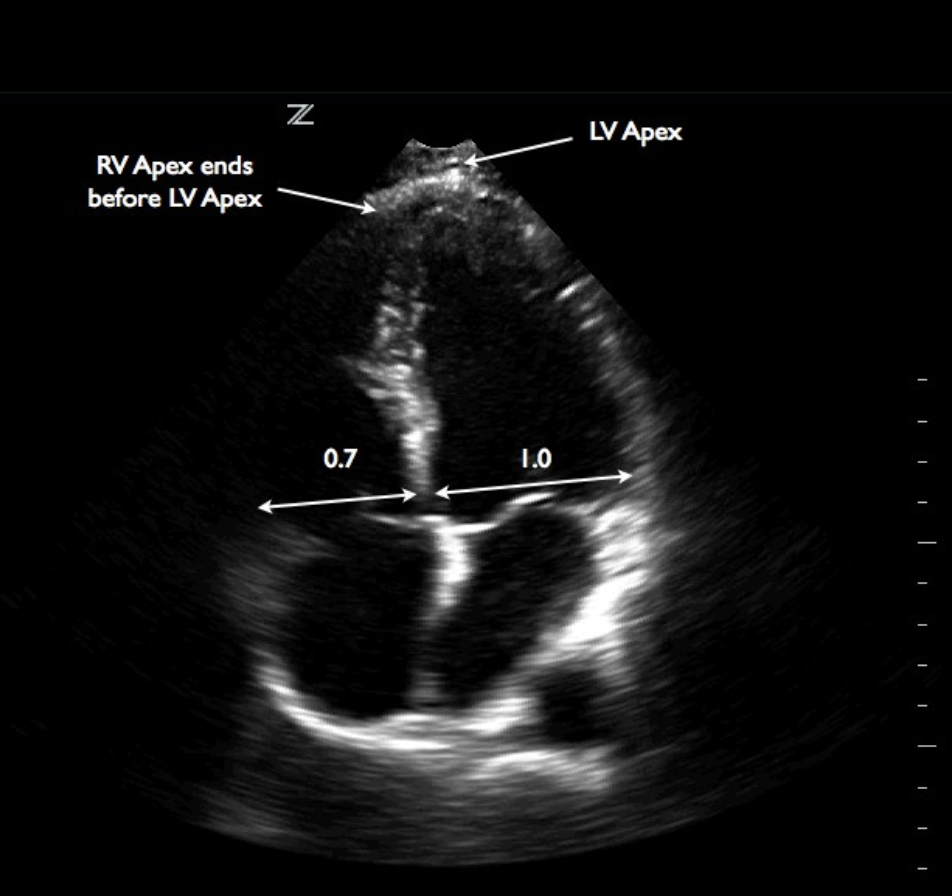
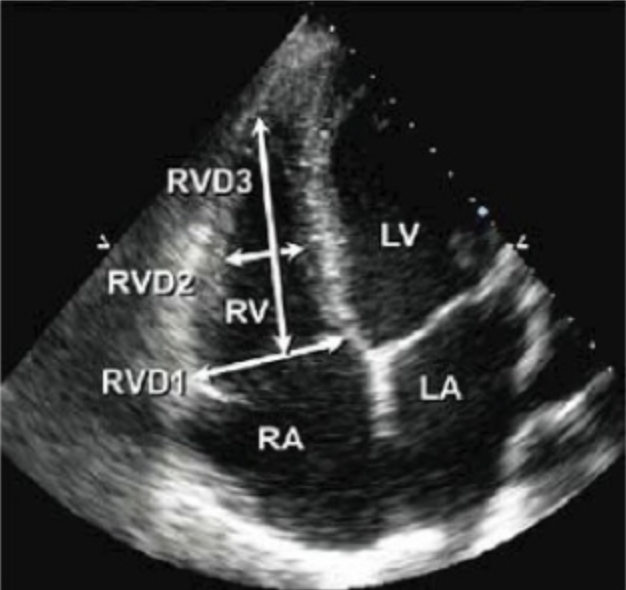
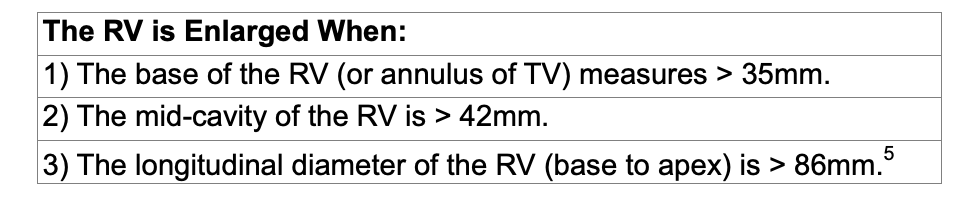
Measure RV:
-
Width above annulus and mid-ventricle
-
Apex to annulus length
-
Functional Measures
-
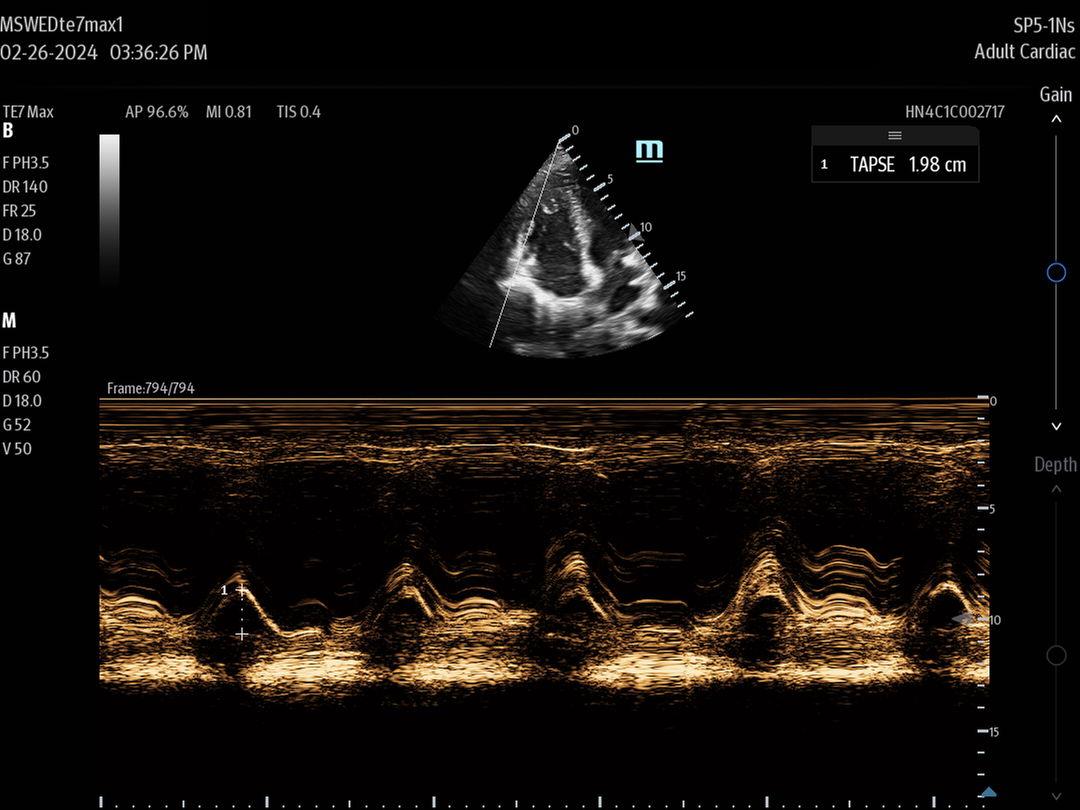
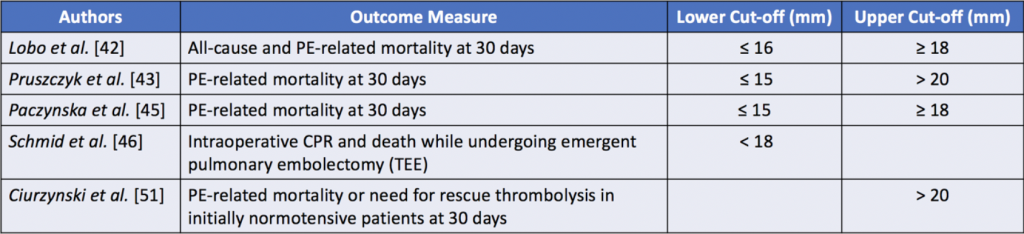
TAPSE (Tricuspid Annular Plane Systolic Excursion):
-
<17 mm = RV dysfunction
-
<14 mm = poor prognosis
-
-
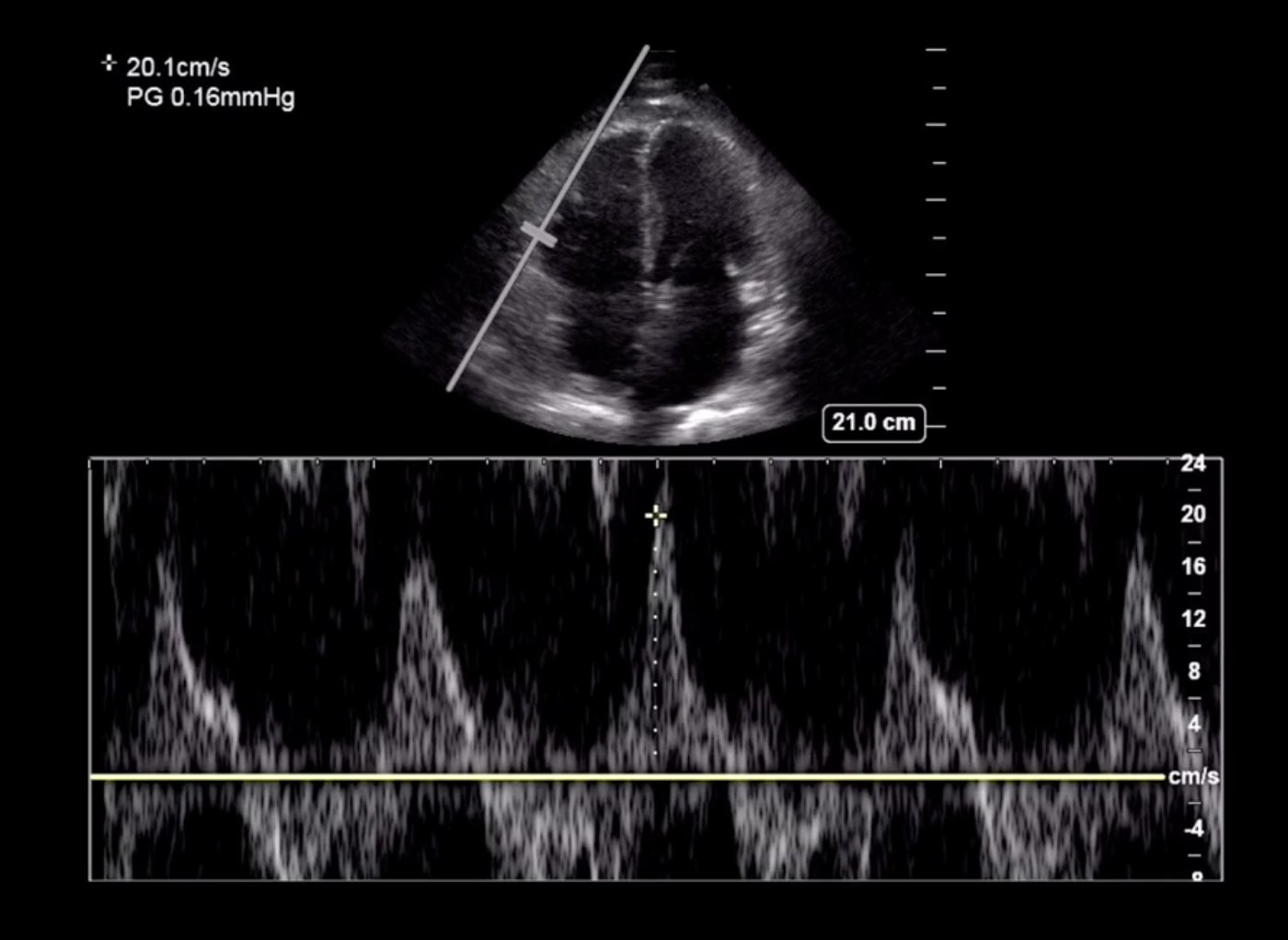
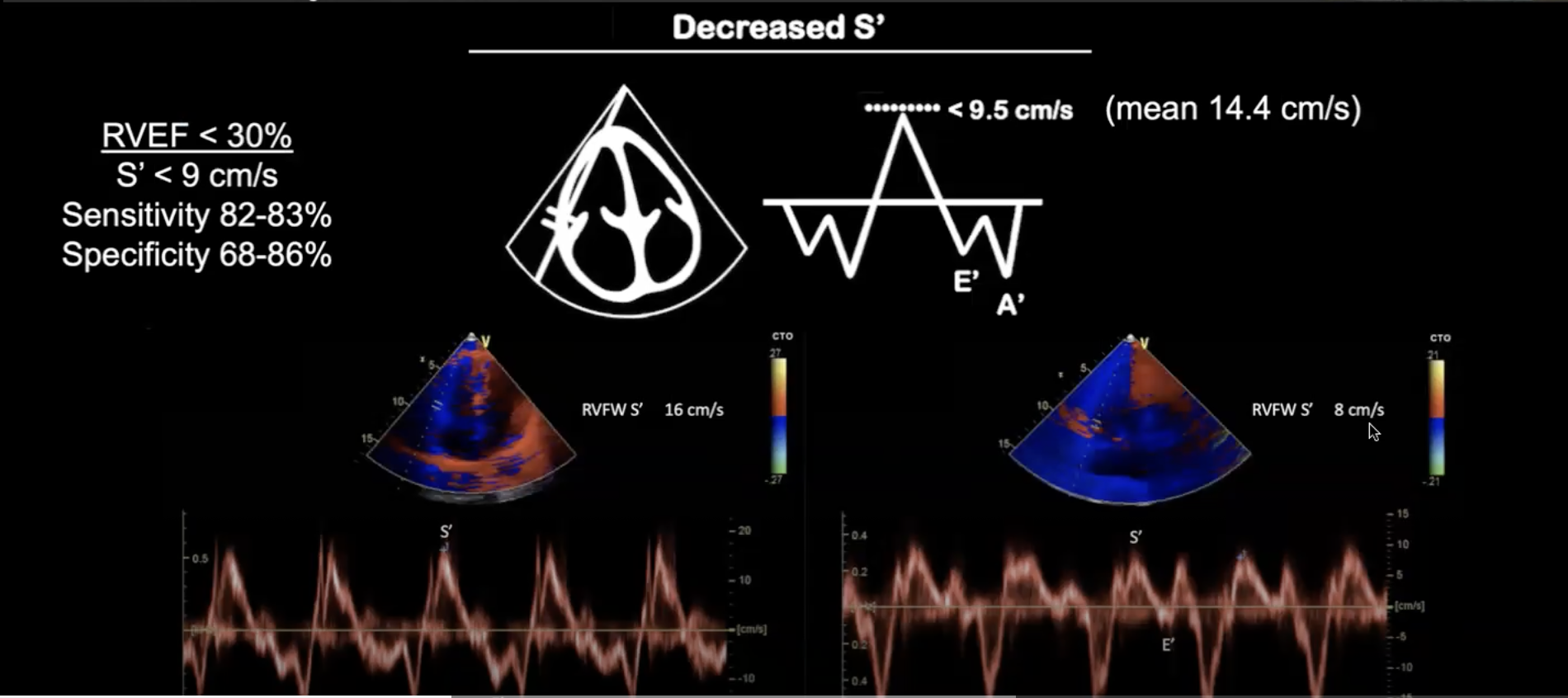
S' (Systolic Excursion Velocity) via Tissue Doppler:
-
10 cm/s = normal
Right Heart
🫁 Pulmonary Circulation & Volume Status
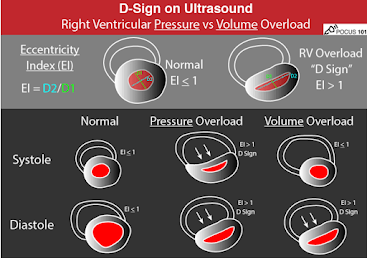
Eccentricity Index (EI)
-
Differentiates pressure overload (PE, pHTN) from volume overload (MTP, CHF)
-
EI seen in parasternal short axis view: flattened septum suggests pressure overload
Pulmonary Artery Systolic Pressure (PASP)
-
PASP = RVSP + RAP
-
RVSP = 4v² (where v = peak TR velocity)
-
RAP estimated by IVC size/collapsibility
-
IVC >2.1 cm & <50% collapse → RAP ~15 mmHg
-
-
-
PASP >36 mmHg = abnormal
⏱️ 60/60 Sign (Suggestive of Pulmonary Embolism)
-
PASP <60 mmHg
-
Pulmonary Acceleration Time (PAT) <60 ms
-
Measure via PW Doppler in RVOT
-
94% specificity for PE when both <60
-
🩸 Pathology Recognition
Pulmonary Embolism
-
TAPSE ↓, 60/60 sign, Eccentricity Index
-
McConnell’s sign not specific (also seen in pHTN, ARDS, RV MI)
Cardiac Tamponade
-
RV diastolic collapse (specific, 60% sensitive)
-
RA systolic collapse (94% sensitive)
-
Plethoric IVC, low cardiac output
-
Use M-mode for pulsus paradoxus detection
📸 Extra Views
-
Suprasternal notch: Aortic arch and dissection evaluation
-
Apical 2- & 3-Chamber: Required for Simpson’s method
Comments
Post a Comment